Knee Realignment Osteotomy (High Tibial Osteotomy) HTO
A surgical procedure to correct knee alignment and reduce pressure on damaged joint surfaces
A knee realignment osteotomy is a joint-preserving surgical procedure designed to shift the weight-bearing axis of your leg away from a damaged or arthritic part of the knee. It may be considered if you have early to moderate osteoarthritis affecting only one side of the knee, particularly the inner (medial) compartment, and want to delay joint replacement surgery.
The most common form of knee realignment is the high tibial osteotomy (HTO), which involves reshaping the upper part of the tibia (shinbone) to correct bow-legged alignment and offload pressure from the medial side of the knee. Other types of osteotomy, such as distal femoral osteotomy (DFO), may be used when the outer side of the knee is affected or when knock-kneed alignment needs to be corrected.
These procedures aim to relieve pain, improve function, and help you stay active by preserving your natural knee joint for as long as possible.
HOW THE KNEE REALIGNMENT OSTEOTOMY WORKS
A knee realignment osteotomy adjusts the alignment of your leg to shift weight away from the worn or arthritic part of the knee joint. This relieves pressure on the damaged area and redistributes forces through the healthier cartilage, helping to reduce pain and slow the progression of arthritis.
This joint-preserving approach can improve knee function and delay or avoid the need for total knee replacement in selected patients.

This procedure may be considered if you:
Have medial or lateral compartment knee arthritis (one-sided wear)
Are under 60 years old and wish to delay joint replacement
Remain physically active and want to preserve your natural joint
Have a bow-legged or knock-kneed alignment that contributes to uneven joint loading
Experience knee pain with activity but have good range of motion and no instability
The biomechanics behind the procedure:
When your knee alignment is off, such as being bow-legged (varus) or knock-kneed (valgus)—the joint experiences uneven loading. A realignment osteotomy shifts your weight-bearing line towards the healthier side of the knee, reducing stress on the worn compartment.
Depending on where the deformity is located, the procedure involves a controlled cut in either the tibia (in a high tibial osteotomy) or the femur (in a distal femoral osteotomy). Realigning these bones changes how they meet at the knee, improving joint mechanics and motion.
Dr Antony Liddell uses detailed imaging and alignment measurements to determine the exact degree of correction needed. This personalised planning ensures the procedure is tailored to your unique anatomy and pattern of joint wear.
A wedge of bone is either removed (closing wedge osteotomy) or a space is created and opened (opening wedge osteotomy) to realign the leg. The bone is stabilised in its new position using a plate and screws, allowing it to heal in proper alignment.
The new alignment reduces pressure on the affected side of the knee, which may:
- Relieve pain and stiffness
- Improve overall knee movement and function
- Protect remaining cartilage and joint surfaces
- Slow the progression of osteoarthritis
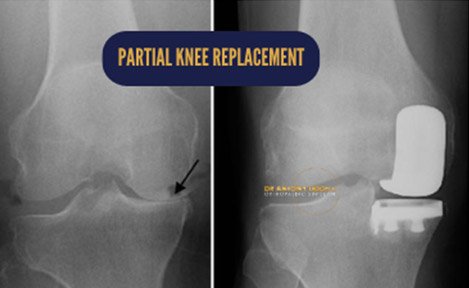
REALIGNMENT OSTEOTOMY VS. PARTIAL KNEE REPLACEMENT
For certain patients, particularly younger individuals with knee malalignment or early-stage arthritis, a high tibial osteotomy can be a preferable option over partial knee replacement. The osteotomy realigns the knee joint by creating an opening in the upper portion of the tibia, which shifts the weight-bearing load away from the damaged cartilage and onto the healthier side of the knee. This allows patients to maintain an active lifestyle with fewer restrictions compared to a knee replacement.

For certain patients, particularly younger individuals with knee malalignment or early-stage arthritis, a high tibial osteotomy can be a preferable option over partial knee replacement. The osteotomy realigns the knee joint by creating an opening in the upper portion of the tibia, which shifts the weight-bearing load away from the damaged cartilage and onto the healthier side of the knee. This allows patients to maintain an active lifestyle with fewer restrictions compared to a knee replacement.
THE REALIGNMENT OSTEOTOMY (HTO) SURGICAL PROCEDURE
A knee realignment osteotomy is a carefully planned and precise operation that involves several key steps to ensure a successful outcome. Dr Liddell uses advanced imaging, customised surgical guides, and proven techniques to achieve the correct alignment for each individual patient. Below is an overview of what happens during the procedure, from pre-operative preparation through to fixation of the bone in its new position.
- Pre-operative planning – The first step in a realignment osteotomy involves thorough pre-operative planning. Dr Liddell will organise X-rays and CT scans to accurately determine the degree of correction needed for your knee. This imaging data is crucial in designing a custom-made jig that will guide the surgical procedure.
- Bone cuts made (osteotomy) –During the surgery, the custom-made jig is applied to the tibia (or femur if necessary), allowing Dr Liddell to make precise cuts in the bone near the knee joint. The location of these cuts is critical for achieving the correct realignment of the knee.
- Change in the bone alignment | Open wedge osteotomy: In an open wedge osteotomy, a wedge-shaped implant is inserted into the tibia after the initial bone cut. This widens the tibia, reducing pressure on the medial (inner) compartment of the knee. This technique is particularly effective for patients with more severe arthritis or those with a knock knee deformity. In some cases, it may be combined with a distal femoral osteotomy to correct more complex alignment issues.
- Change in the bone alignment | Closed wedge osteotomy: In a closed wedge osteotomy, after the initial osteotomy (bone cut), Dr Liddell removes a wedge-shaped piece of bone from the tibia. This shifts the alignment of the tibia relative to the femur, effectively redistributing the weight load across the knee joint. This technique is often used when less severe correction is needed.
- Fixation of the osteotomy – Once the desired alignment is achieved, the osteotomy is secured using a metallic plate and screws to hold the bone in its new position. In an open wedge osteotomy, a bone graft may be used to fill the gap at the osteotomy site, particularly if a significant correction has been made.
RECOVERY FOLLOWING REALIGNMENT OSTEOTOMY
The recovery timeline following a high tibial osteotomy (HTO) can vary depending on factors such as the extent of cartilage damage, the presence of knee arthritis, the patient’s overall health, and the specifics of the surgical procedure. Generally, patients should anticipate a recovery period that includes 6 to 12 weeks of physiotherapy, with full recovery expected between 3 to 6 months.
For patients with osteoarthritis, an HTO can effectively delay the need for a knee replacement, with the benefits often lasting at least 10 years in 8 out of 10 patients.
At this stage, the wound dressings will be removed, and the surgical site will be carefully examined to ensure proper healing. Any sutures will also be removed during this visit.
It’s crucial to keep the wound dry for the first two weeks following surgery. After your wound has been reviewed at the 2-week post-operative consultation, you may begin showering without dressings. Pool-based rehabilitation or swimming should be avoided for at least 4 weeks after surgery to minimise the risk of infection.
You will need to use crutches for weight-bearing support until approximately 4 weeks post-op. If you have a desk-based job, plan for 3 to 4 weeks of leave to allow for sufficient recovery.
At the 8-week mark, the range of motion in your knee will be assessed. By this time, it is expected that you will be able to fully straighten your knee and achieve a bend of more than ninety degrees.
A special X-ray will be taken from the hip to the ankle to confirm that the alignment of your knee has been successfully corrected, along with another X-ray of the knee to check on the healing progress at the osteotomy site.
While complete healing of the osteotomy is not expected at this stage, it’s important to note that driving should not be resumed until at least 6 weeks post-op. Before driving, you must be off strong pain medications, able to walk without crutches, and have a relatively pain-free range of motion in the affected knee.
Around 4 months after surgery, an X-ray will again be taken to further assess the healing of the osteotomy site. By this time, your knee should have regained its full range of motion, although some residual swelling may still be present.
At approximately 8 months post-op, a final X-ray will be conducted to ensure that the osteotomy site has fully healed. At this stage, you may begin to gradually return to sports and other high-impact activities, typically between 6 to 8 months after surgery.
Dr Liddell will also discuss the potential benefits of removing the osteotomy plate at this point. Although plate removal is not mandatory, it is often recommended, especially if the plate causes discomfort or is prominent under the skin. The plate is designed to be robust and withstand the force of your body weight, but in some cases, it can be felt through the incision site, which may cause discomfort.
If further knee surgery is required in the future, such as a knee replacement, the presence of the plate can complicate the procedure. Removing the plate several years after surgery can also be more challenging due to bony ingrowth and overgrowth. It is therefore typically performed 9 to 12 months after the initial surgery once the osteotomy site has completely healed.
Plate removal is relatively straight forward and is usually an outpatient procedure, meaning you won’t need to stay overnight in the hospital.
Knee realignment osteotomy is a joint-preserving surgical option that may help reduce pain, improve function, and delay the need for knee replacement in selected patients. By correcting leg alignment and offloading the damaged area, it aims to support a more active lifestyle and protect your natural knee joint. Dr Antony Liddell will assess whether this procedure suits your individual anatomy and long-term goals.